
The prevalence of single-sided or unilateral hearing loss (UHL) in school-aged children may be as high as 5%. Historically, unilateral hearing loss was thought to have little consequence because speech and language presumably developed appropriately with one normally hearing ear.
According to Washington University pediatric otolaryngologist Judith Lieu, MD, however, some studies suggest that a significant proportion (22-59%) of children with UHL may have educational and/or behavioral problems, compared to their normally hearing peers. Dr. Lieu’s research program has been shedding light on this problem and is helping to identify those children that might benefit from amplification or other types of intervention.
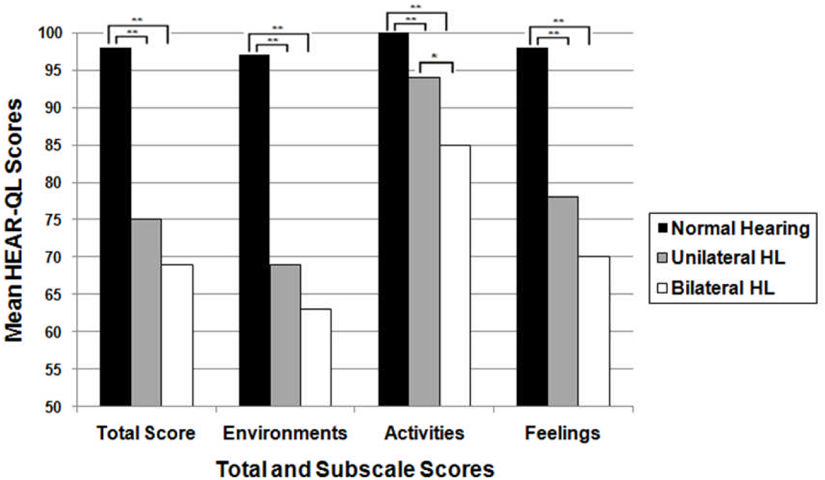
“We are interested in investigating the outcomes that go beyond the audiogram,” explained Lieu. “Speech-language development is obviously an important outcome, but we are also interested in assessing quality of life, fatigue and cognition. One of the most important developments to come from these studies is a survey called the HEAR-QL, Hearing environments and reflection on quality of life.”
The original HEAR-QL, designed for children 7-12 years old, is a 26-question survey that collects evaluations of three factors: difficulty hearing in certain environments/situations; impact of hearing loss on social/sports activities; and impact of hearing loss on child’s feelings. A subsequent design for older children assesses more social aspects related to family and friends and the school environment.
The questionnaire has now been validated for three age groups: 2-6 years, 7-12 year, and 13-18 years. It has been shown to be more sensitive than previous pediatric quality of life surveys at identifying children with hearing loss and helping to evaluate useful interventions.
“Quality of life surveys can document important aspects of living with hearing loss beyond a quantitative measure of hearing ability,” said Lieu. “If we can identify how a child perceives the effects of their hearing loss, then we can help the clinician determine where intervention is warranted in order to improve the child’s overall being.”
The HEAR-QL has now been translated into nine languages: Arabic, Dutch, German, Marathi, New Zealand English, Japanese, Taiwanese, Mandarin, and Turkish. Other translations are in the works.
Most of these translations are for studies led by audiologists, speech-language pathologists, or otolaryngologists. The National Cancer Institute Children’s Oncology Group is planning to use it to help track late-effects outcomes in children who have survived childhood cancers.
If you are considering or interested in using these assessments and would like more information, please contact Dr. Judith Lieu.